Road Traffic Noise, Public Health, and the Urgent Case for India
By Dr. Manish Manohare
Noise pollution is increasingly recognized as a major environmental determinant of health. While air pollution receives sustained policy attention, environmental noise remains comparatively under-prioritized despite mounting scientific evidence of its impact. Road traffic noise, in particular, has emerged as one of the leading environmental stressors in urban settings. In global burden assessments, it ranks second among environmental risks in terms of health impact in many developed regions (World Health Organization [WHO], 2011).
India’s rapid urbanisation, expanding vehicle fleet, and heterogeneous traffic systems have created complex and high-intensity acoustic environments. Yet systematic assessment of noise-related health burden in India remains limited. Understanding the scale of risk requires first examining what global evidence reveals about the relationship between noise and health.
Noise and Health: The Scientific Evidence
The health impacts of traffic noise are broadly classified into auditory and non-auditory effects. Auditory impacts include noise-induced hearing loss, tinnitus, hyperacusis, and speech interference. Sustained exposure above 85 dB for prolonged durations can cause permanent hearing impairment. However, in environmental contexts, the more pervasive impacts are non-auditory (Figure 1).
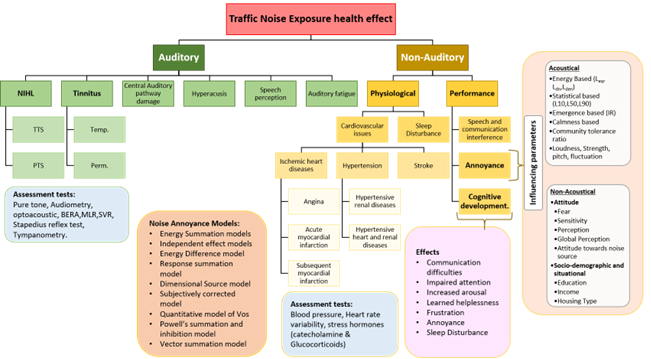
Figure 1: Traffic Noise and its Health impact
(Image adopted from Manohare, M., Rajasekar, E., Parida, M. & Vij, S. (2022). Bibliometric analysis and review of auditory and non-auditory health impact due to road traffic noise exposure. Noise Mapping.)
Chronic exposure to traffic noise activates stress-response systems. Repeated stimulation of the autonomic nervous system and the hypothalamic-pituitary-adrenal axis leads to elevated cortisol levels, increased blood pressure, endothelial dysfunction, and long-term cardiovascular strain (Babisch, 2014; Münzel et al., 2018). Over time, this physiological activation increases the risk of hypertension, ischaemic heart disease, stroke, and metabolic disorders.
The World Health Organization estimates that more than two billion people worldwide are exposed to environmental noise above 55 dB, a level associated with adverse health outcomes (WHO, 2018). In Europe, environmental noise contributes annually to approximately 61,000 disability-adjusted life years (DALYs) due to ischaemic heart disease, 45,000 due to cognitive impairment in children, 903,000 due to sleep disturbance, and 654,000 due to annoyance (WHO, 2011). The European Environment Agency estimates around 10,000 premature deaths annually linked to environmental noise exposure (European Environment Agency [EEA], 2020).
Sleep disturbance is a particularly important pathway. Night-time noise exposure above 55 dB has been linked to fragmented sleep architecture and reduced restorative sleep (WHO, 2009). Chronic sleep disruption contributes to obesity, diabetes, impaired immunity, and reduced cognitive performance. Evidence also suggests that even small reductions in environmental noise can yield measurable health benefits. In Madrid, a 1 dB reduction in traffic noise was associated with 200 to 300 fewer deaths annually from cardiovascular and respiratory causes (Recio et al., 2016).
Exposure-response relationships have been fundamental in quantifying these risks. Schultz (1978) first synthesised social surveys to model the relationship between noise exposure and community annoyance. Miedema and Oudshoorn (1998) later refined these relationships using the Lden metric to estimate the percentage of highly annoyed populations. These models underpin modern noise policy and burden-of-disease calculations in Europe.
The scientific consensus is therefore clear: environmental noise is biologically active, cumulative in effect, and associated with measurable health outcomes.
Severity of the Noise Scenario in India
If European cities, operating under regulated traffic systems, experience such burdens, the implications for India are significant. Indian urban traffic differs fundamentally from homogeneous Western systems. It is characterised by heterogeneous vehicle fleets, irregular acceleration and braking patterns, minimal lane discipline, and pervasive horn usage (Figure 2). These features create highly variable, impulsive, and spectrally complex sound environments.

Figure 2: Typical traffic condition on Indian streets. (source: author)
The United Nations Environment Programme identifies road traffic as the dominant contributor to urban noise in Indian cities. Several studies recorded peak levels in cities such as Moradabad (114 dB), Kolkata (89 dB), Jaipur (84 dB), and New Delhi (83 dB) substantially exceed WHO recommended thresholds and India’s Central Pollution Control Board (CPCB) limits. CPCB guidelines prescribe 65 dB(A) for commercial areas and 55 dB(A) for residential areas during daytime, yet violations are frequently documented.
Community-level studies illustrate the magnitude of exposure. Agarwal and Swami (2011) reported equivalent continuous sound levels between 73 and 86 dB(A) across surveyed locations in Delhi. Within this population, 52 % reported frequent irritation, 46 % reported hypertension, and 48.6 % reported sleep disturbance. These prevalence rates suggest that noise exposure may be contributing significantly to cardiovascular and stress-related conditions in Indian cities.
Figure 3: Noise measurement in New Delhi, (source : author)
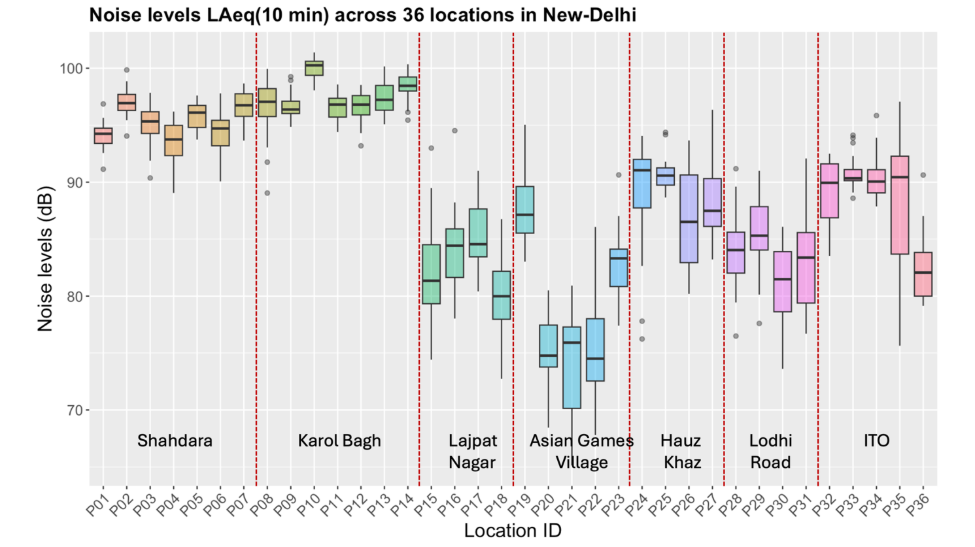
Figure 4: Noise levels across different location in New-Delhi, India (source: author)
In addition to previously reported surveys, daytime field measurements conducted by the author across multiple arterial and sub-arterial streets in New Delhi (Figure 3) show that most monitored locations recorded equivalent sound levels well above CPCB permissible limits (Figure 4). The spatial distribution of these measurements highlights persistent exceedance across commercial corridors and mixed residential zones, reinforcing the chronic nature of urban exposure conditions in the capital city.
Importantly, conventional energy-based metrics such as LAeq may not adequately capture the health-relevant characteristics of heterogeneous traffic noise. Research in Indian contexts demonstrates that psychoacoustic parameters such as loudness, sharpness, and roughness may better explain perceived annoyance and physiological response (Manohare et al., 2022). Experimental studies incorporating psychophysiological monitoring have observed measurable reductions in heart rate variability during exposure to heterogeneous traffic noise, indicating autonomic imbalance and stress response activation.
Short-term exposure studies further reinforce these findings. Environmental noise can trigger immediate physiological responses including increased heart rate and skin conductance (Rylander, 2004; Li et al., 2023). Individuals with high noise sensitivity show amplified responses under identical exposure conditions (Stansfeld et al., 2021). These findings are particularly relevant in dense Indian urban environments where populations are exposed not only during transit but continuously in residential settings located directly adjacent to arterial roads.
Despite these indicators, India lacks comprehensive longitudinal cohort studies linking traffic noise exposure to cardiovascular morbidity or mortality. Noise mapping efforts often rely on adapted European prediction models that may not fully represent heterogeneous traffic dynamics. Consequently, national burden estimates remain uncertain.
Policy and Intervention Pathways
Addressing noise pollution in India requires a multi-layered approach spanning research, regulation, planning, and public awareness.
First, India-specific noise emission and propagation models must be developed. Heterogeneous traffic systems require prediction frameworks that account for mixed vehicle categories, acceleration variability, and horn events. Without accurate exposure mapping, prioritisation and intervention planning remain weak.
Second, systematic urban noise monitoring networks should be established. Continuous monitoring, rather than periodic spot measurements, can provide actionable data for municipalities and regulatory agencies.
Third, vehicle noise emission standards must be strengthened and enforced. This includes regulation of horn design and usage. Transitioning toward electric mobility, particularly in public transport and two-wheeler segments, offers long-term noise reduction benefits at urban speeds.
Fourth, urban planning policies should incorporate acoustic considerations. Setback distances for residential developments near major corridors, façade insulation standards, and barrier designs must be integrated into development control regulations.
Fifth, health surveillance systems should incorporate environmental noise exposure metrics. Integrating noise exposure into cardiovascular and metabolic disease research will allow more accurate burden estimation and targeted interventions.
Finally, public awareness is essential. Noise is often perceived as an unavoidable by-product of urban life. Framing it as a preventable health risk can catalyse behavioural change, including reduced horn usage and community-driven monitoring initiatives.
Conclusion
The global evidence is unequivocal: road traffic noise contributes to cardiovascular disease, sleep disturbance, cognitive impairment, and hearing loss. In India’s dense and heterogeneous urban environments, exposure levels frequently exceed recommended thresholds. Emerging national research indicates measurable physiological stress responses under such exposure conditions.
Noise pollution is not a minor urban inconvenience. It is a structural environmental health risk. As India continues to urbanise and motorise, the acoustic burden will intensify unless addressed through coordinated scientific, regulatory, and planning interventions.
Recognising noise as a public health priority is the first step. Acting upon it with data-driven policy and context-specific solutions is the necessary next step.
References
Agarwal, S., & Swami, B. L. (2011). Development of a noise prediction model under interrupted traffic flow conditions: A case study for Jaipur City. Noise & Health, 13(55), 402–407.
Babisch, W. (2014). Updated exposure-response relationship between road traffic noise and coronary heart diseases. Noise & Health, 16(68), 1–9.
European Environment Agency. (2020). Environmental noise in Europe – 2020. EEA Report No 22/2019.
Li, X., et al. (2023). Short-term physiological responses to environmental noise exposure. Science of the Total Environment, 858, 159862.
Manohare, M., et al. (2022). Noise pollution in heterogeneous transportation systems: Implications for health and perception in Indian cities. Noise & Health, 24(115), 12–21.
Miedema, H. M. E., & Oudshoorn, C. G. M. (1998). Annoyance from transportation noise: Relationships with exposure metrics DNL and Lden. Journal of the Acoustical Society of America, 104(6), 3432–3445.
Münzel, T., et al. (2018). Environmental noise and the cardiovascular system. Journal of the American College of Cardiology, 71(6), 688–697.
Recio, A., et al. (2016). Road traffic noise effects on cardiovascular and respiratory mortality. Environmental Research, 150, 193–199.
Rylander, R. (2004). Physiological aspects of noise-induced stress. Journal of Sound and Vibration, 277(3), 471–478.
Schultz, T. J. (1978). Synthesis of social surveys on noise annoyance. Journal of the Acoustical Society of America, 64(2), 377–405.
Stansfeld, S. A., et al. (2021). Noise sensitivity and health effects. International Journal of Environmental Research and Public Health, 18(3), 1–14.
World Health Organization. (2009). Night noise guidelines for Europe. WHO Regional Office for Europe.
World Health Organization. (2011). Burden of disease from environmental noise: Quantification of healthy life years lost in Europe. WHO Regional Office for Europe.
World Health Organization. (2018). Environmental noise guidelines for the European region. WHO Regional Office for Europe.
Author Details:
Dr. Manish Manohare is an environmental acoustician and urban noise researcher specialising in psychoacoustics, soundscape studies, and traffic noise modelling. His work integrates acoustic measurements with psychophysiological analysis to examine the health impacts of heterogeneous transportation systems in Indian cities. He currently serves as Assistant Professor at IIT Delhi, focusing on environmental noise and public health research.